Diseases with an upside.
By Rich Feldenberg

Since life’s earliest emergence on planet earth, disease has been our constant and unwelcome companion. Even the first single celled organisms were susceptible to break down, nutritional deficiencies, and harmful genetic mutation. When single celled life upgraded to the multicellular stage, finally becoming large, it was then susceptible to a host of new disorders, such as cancer that interfered with the organization and growth of cells that now had to survive as part of a collective. Humankind is no different than the rest of the animal kingdom in this regard, and throughout human existence disease has lead to untold suffering, death, and at times the threat of total extinction. It may therefore be surprising to learn that some diseases confer protection against other types of illness, and this seems to account for the high prevalence of some of these disorders in the human population. If the protective benefit of the disease mutation on a large portion of the population outweighs the suffering and death of a small portion of the population, natural selection will swing the balance in favor of keeping those mutations in the gene pool. Not only may the disease mutation simply persist in the gene pool, but it may become very prevalent because it is selected for in the right environment, where the other illness it protects against is a major threat. To illustrate how this works I’ll give some detail on two well known examples of diseases and their upside - in other words, how they protect against other threats to our species.
The first example is that Sickle Cell Anemia (SCA), which has the best documented evidence as to its evolutionary risk versus benefit ratio in its effected population. Sickle Cell Anemia is a genetic disease that causes anemia (low red blood cell counts), and can lead to painful, and potentially deadly pain crises. It is inherited as an autosomal recessive trait - meaning that if you receive one copy of the mutated gene from each of your parents, then you have two abnormal copies of the gene (are homozygous, in the language of genetics) and will have the disease. Each of your parents, however, has only one mutant copy and also one normal copy (is heterozygous), and so is only a carrier (has sickle cell trait) and will not show symptoms of the disease under normal circumstances.
SCA is due to a single base switch in the DNA that codes for the beta-chain of the hemoglobin molecule. Adult hemoglobin is made of two alpha chains and two beta chains. This is the major oxygen carrying protein in the blood, although, there are other versions of hemoglobin that are produced (one example is fetal hemoglobin with two alpha chains and two gamma chains). In SCA, there is a substitution of the amino acid glutamic acid for valine at the 6th amino acid in the beta chain. Since valine is more hydrophobic than glutamic acid this has the unfortunate consequence of causing the hemoglobin molecules to polymerized and compact together, deforming the shape of the red blood cells (RBCs) that carry them, into a sickle shape - hence the name Sickle Cell Anemia. The polymerization event is more likely to happen if the affected individual is dehydrated, in a low oxygen state (hypoxic), or otherwise ill with another illness. The deformed red blood cells can not get through the tiny capillaries very well, causing blockages that deprive tissues of blood and oxygen. The result is pain and organ damage.

Over time, people with SCA damage their spleen so badly that they lose the its important immune function, which normally you against encapsulated bacterial infections. These are certain bacteria that are surrounded by a polysaccaride capsule, that helps them to escape detection by the immune system. Someone without a functioning spleen can then die of these types of infections, whereas those with normal spleens would be able to fight off the infection easily. The blockages to blood flow due the abnormal sickle shaped RBCs can lead to strokes and to Acute Chest Syndrome. If people with SCA become infected with the common virus Parvovirus B19, they can develop severe life threatening anemia, with hemoglobin levels that get so low they can develop heart failure.
Sickle cell anemia is common in sub-Saharan Africa, and about 300,000 are born with disease each year. All the complications of SCA listed above can be fatal so why would this disorder have such a high prevalence? The answer seems to be that although people with full blown Sickle Cell Anemia are at a most definite disadvantage from a survival aspect, those who are carriers of SCA are protected against another common killer - Malaria. Malaria is an infectious disease caused by the protozoan Plasmodium. It has a complex life cycle, part of which is spent inside the mosquito Anopheles, and part is spent inside a vertebrate host - such as a human. When an infected female mosquito bites a human, the organism is transmitted into the persons blood stream where it travels to the liver, infects liver cells, reproduces, and then is released back to the bloodstream where it infects RBCs. The symptoms of Malaria include fever, vomiting, joint and muscle pain, headache, and in some cases seizures. As the Plasmodium organism goes through its life-cycle within the host, from liver to RBC and back again (these are known as the liver phase and the erythrocytic phase respectively), the symptoms return in a cyclical fashion. In some cases the organism passes through the blood-brain barrier leading to Cerebral Malaria, which is a very serious complication. Malaria has a high mortality rate if untreated - as would have been the case before the age of modern medicine.

It was observed, early on, that in regions endemic to malaria, people who were carriers of the sickle cell mutation showed resistance to the malaria infection, and that full blown SCA has a high prevalence in those same regions where malaria is endemic. Further studies confirmed that those individuals who are carries for the sickle cell mutation, do in fact, enjoy a protection due to their gene mutation. Unfortunately, those with actual sickle cell anemia (homozygous for the gene mutation) are not protected against malaria. Not only do they have to suffer the fate of SCA, but if they get malaria they have a worse prognosis because the malaria damages their already vulnerable RBCs.

For a long time it was thought that sickle cell trait most likely confers its malarial protection by making it difficult for Plasmodium organisms to infect the abnormally shaped RBCs, and that the abnormal RBCs are removed more readily by circulating macrophages, helping to rid Plasmodium infected cells more readily. More recent research seems to suggest that the protective mechanism is more complex that that, and involves the up regulation of an enzyme called heme oxygenase-1(HO-1). HO-1 causes the breakdown of heme, and the release of carbon monoxide (CO), iron, and biliverdin, resulting in an anti-inflammatory effect. HO-1 is upregulated or produced to a greater extent in RBCs that have the abnormal hemoglobin associated with SCA, and it is the production of CO that seems to have a detrimental effect for the Plasmodium organisms. It confers protection against cerebral malaria, and decreased mortality for those with sickle cell trait who become infected with malaria. This might also be the answer to why several other diseases or disease traits have also been observed to offer protection against malaria, such as thalassemia trait and Glucose-6-Phosphate Deficiency. These disorders might also increase the activity of HO-1.
We’ll move now to another deadly disease that seems to have remained in the population because it offered a survival advantage. This is the kidney disease called Focal Segmental Glomulosclerosis (a real mouthful) or just plain old FSGS for short. FSGS can be caused by chronic infections, such as hepatitis or HIV, but many cases are due to a genetic mutation. It is a subset of the genetic form that may have been selected for to protect against Sleeping Sickness. In FSGS the tiny filters in the kidneys, called glomeruli, become scarred until they can no longer filter. This can eventually progress to kidney failure and the need for dialysis or kidney transplant. Kidney failure is fatal without modern medical care and FSGS is one of the more common causes for young people to be on dialysis. Its also, often more common and resistant to therapy in African Americans and other people of African descent.
Some people with the genetic form of FSGS have a mutation in a gene called APOL1, and if you are an individual with two mutated copies of the APOL1 gene, your risk of developing FSGS and kidney failure is 17 times higher than if you have two normal copies of the gene. That adds up to around a 4% chance of developing FSGS over your lifetime if you are homozygous for mutant APOL1. This mutation is also thought to explain 18% of all cases of FSGS that currently exist. There are two types of mutations in the APOL1 gene that can increase risk for FSGS kidney disease. These is the G1 variant, which contains two amino acid substitutions - one is a replacement of glycine for serine at amino acid 342 in the protein (S342G), and the other switch is a replacement of methionine for isoleucine at amino acid 384 in the protein (I384M). You have to have both of these switches you have the G1 variant. The other variant is the G2 variant where 6 base pairs are deleted in the DNA coding for APOL1 starting at base 388. People can have either a G1 variant or a G2 variant, but never have both types.
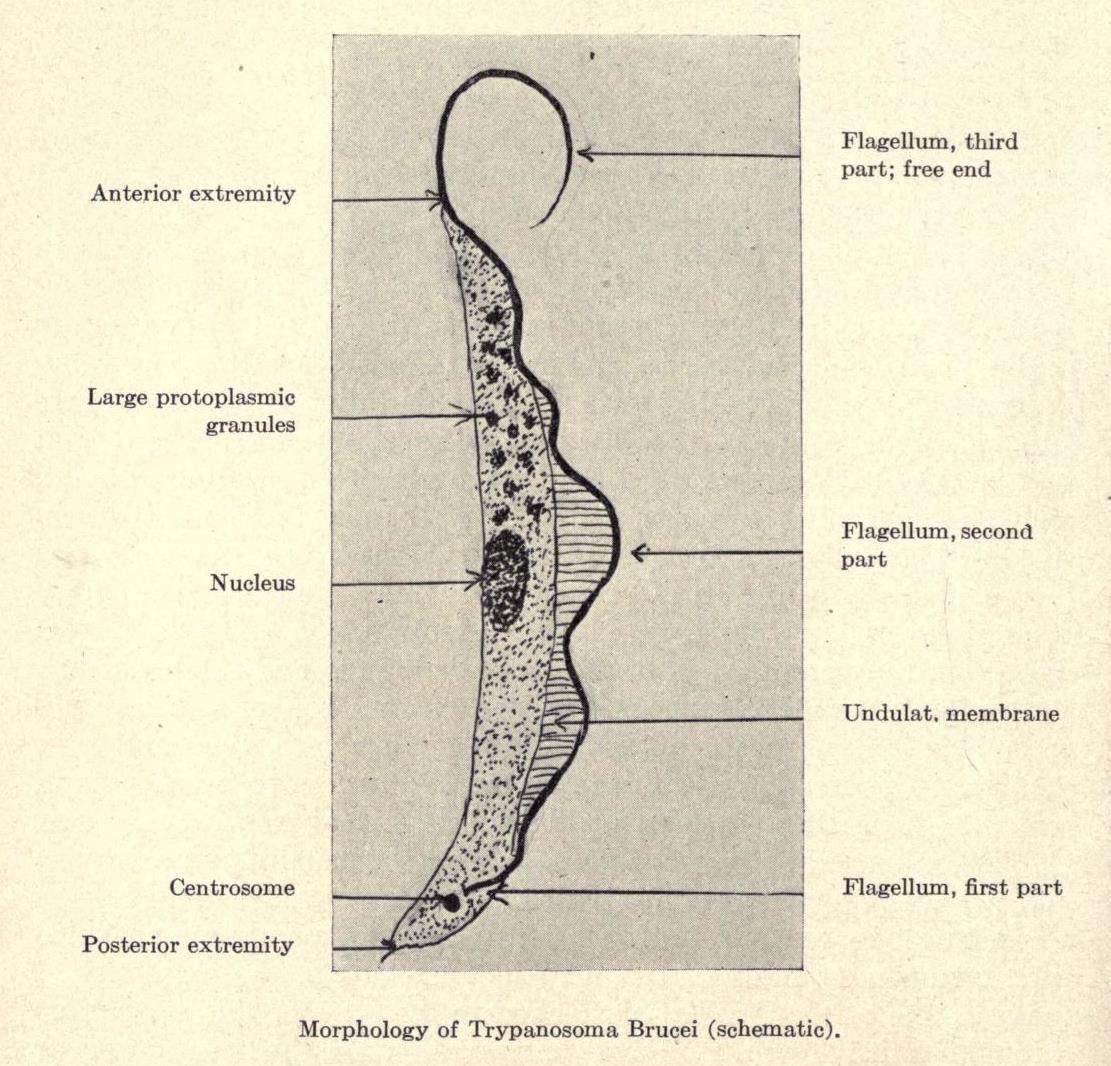
APOL1 is a protein that circulates in the blood and is part of the high-density lipoprotein (HDL - otherwise known as the “good” cholesterol). Exactly how the mutated form of APOL1 causes kidney disease is still not known. What is known, however, is that those individuals with either a G1 or G2 specific gene mutation in APOL1 have protection against African Sleeping Sickness, caused by the protozoan Trypanosoma brucei. This tiny single celled eukaryotic organism is transmitted to its human host by the bite of the tsetse fly. It is a common and dangerous disease in sub-Saharan Africa. In 1990 it caused 34,000 deaths, but the death rate dropped to 9000 in 2010, thanks to efforts of the World Health Organization to prevent and treat the infection.
Those affected by the parasite experience two distinct stages of infection. In the first stage the victim develops headaches, fever, and severe itching. This resolves only to eventually progress to the second stage of the disease which effects the central nervous system causing confusion, paralysis, neuromuscular weakness, and sometimes psychiatric illness. There is a reversal of the sleep-wake cycle, giving the disorder its common name. Infected persons often sleep in the day and remain awake at night. Without treatment the disease always ends in the death of its victim. It can be treated with the drug pentamidine, when in the first stage, or drugs such as eflornithine or melarsoprol for second stage disease.

Like the association of Sickle Cell Anemia and malaria, those geographic regions with a high incidence of sleeping sickness also have a high incidence in the population of APOL1 G1 or G2 variants. This is because those gene variants protect against the ravages of the Trypanosomes. The APOL1 variants cause the lysis (breaking apart of the cell membrane) of Trypanosomes that cause sleeping sickness. The normal gene for APOL1 gives us resistance to other species of Trypanosomes that do infect other mammals, but are unable to harm us. The sleeping sickness Trypanosome (Trypanosome brucei rhodesiense) is immune to the normal APOL1 since it has evolved a serum resistance-associated protein (SRA) that blocks a portion of the APOL1 protein, neutralizing its anti-trypanosomal action. Not so for the APOL1 variants G1 or G2, however. They are able to get around this SRA and destroy the parasite. From an evolutionary point of view, the advantage of being more resistant to sleeping sickness in an area of high risk, outweighs the cost of having a higher than average chance of kidney disease. There is no advantage, however, to having these variants if your ancestors originated where sleeping sickness is not a problem, so other populations aren’t found to have these gene mutations.
The two examples of Sickle Cell anemia and Focal Segmental Glomerulosclerosis (APOL1 mutation) are not the only situations where a disease mutation protect us against another illness. I’ll just briefly mention two more. Tay-Sachs disease, which is a lethal neurodegenerative disorder in the homozygous state, seems to protect against Tuberculosis in carriers (heterozygotes). Also Cystic Fibrosis (CF) which usually leads to severe and chronic lung disease in the homozygous state, may have protected against the effects of cholera in the heterozygous carriers. The CF mutation inactivates a chloride channel called CFTR, in the cell membrane. Being a carrier for this mutation may have prevented the lethal dysentery that would have accompanied infectious cholera, by preventing water loss in the intestines due to poorly working chloride channels. It is a very common gene mutation, with 1 in 25 people of European descent being a carrier for the CF gene mutation.
When we think disease we think of the suffering of its victims and the cost to society. We are often unaware of the balance of the many forces involved, which influence why a particular disease may be so common in a given population. The factors involved are typically much more complex than we appreciate, and most of them are still unknown to us. Natural selection is working behind the scenes in ways that are difficult to detect on just a casual examination. It may be of no consolation to the sufferers of a serious disease, or the family members devastated by a loved ones sickness and loss, but natural selection, with its cold blind eye to pain or suffering, seems to have fixed some of this in place to allow more genes to be passed onto future generations. Evolution is not directed toward any particular goal and has no empathy or sense of compassion. It only selects those traits that happen to give the organism the best chance to pass on its genes in its evolved environment. This is where the human mind comes into play. Now that we are finally learning to understand the root causes of disease at the genetic and molecular level, we can work to treat, cure, and eradicate disease. Although we are not there yet, in theory it should be possible to cure a condition like sickle cell anemia with gene therapy. At the same time, we shouldn’t have to worry about worsening the burden of malaria if SCA were eliminated, since we can also work on better therapies to treat the malaria, and more effective strategies to prevent infection with Plasmodium.
References and other reading:
1. “Mystery solved: How sickle hemoglobin protects against malaria”, ScienceDaily; April 29, 2011
2. “Sickle Cell Anaemia and Malaria”, Lucio Luzzatoo, Mediterranean Journal of Hematology and Infectious Disease; Oct. 3, 2012.
3. Sickle Cell disease; Wikipedia.
4. Malaria; Wikipedia.
5. Heme Oxygenase-1; Wikipedia.
6. “APOL1 Genetic Variants in Focal Segmental Glomerulosclerosis and HIV-Associated Nephropathy”, Jeffrey B. Kopp, et al., Journal of the American Society of Nephrology; Nov. 2011.
7. “Association of Trypanolytic ApoL1 Variants with Kidney Disease in African-Americans”, Giulio Genovese, et al., Science, August 13, 2010.
8. “A co-evolutionary arms race: trypanosomes shaping the human genome, humans shaping the trypanosome genome”, Paul Capewell, et al., Parasitology, June 26, 2014.
9. “A risk allele for focal segmental glomerulosclerosis in African Americans is located within a region containing APOL1 and MYH9”, Giulio Genovese, et al., Kidney International, Oct. 2010.
10. African Trypanosomiasis; Wikipedia.
SEO Brisbane
ReplyDeleteSEO company Brisbane
SEO Sydney
SEO company Sydney
SEO Melbourne
SEO company Melbourne
SEO Perth
SEO company Perth
SEO Adelaide
SEO company Adelaide